Find the latest COVID-19 news and guidance in Medscape's Coronavirus Resource Center.
The year 2020 started with American physicians, nurses, and the whole healthcare workforce dispirited, in a deep state of burnout, with the worst rates of clinical depression and suicides that have been recorded. Indeed, this was not confined to the United States; a global epidemic of burnout had been diagnosed. But things were about to get considerably worse for the healthcare workforce.
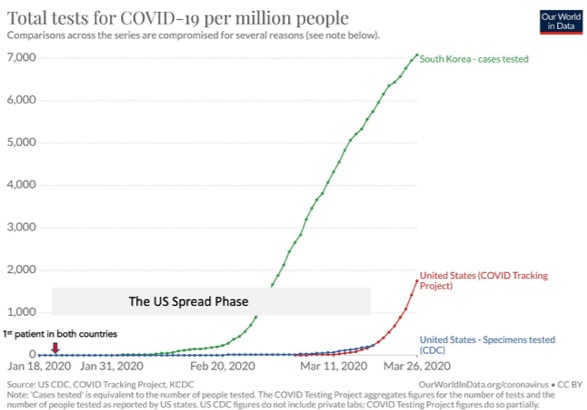
In December 2019 an epidemic of pneumonia, with many fatalities, erupted in Wuhan, China. The pathogen was sequenced and determined to be a novel coronavirus on January 5, 2020, and was subsequently named SARS-CoV-2. The first patient in the United States with COVID-19, the disease caused by SARS-CoV-2, was diagnosed in Seattle on January 21, which was within 24 hours of the first patient diagnosed in South Korea, a key country for comparison (Figure, adapted from Our World in Data).
Figure 1. Testing for COVID-19 in the United States and South Korea
The First Phase: "Silent" US Spread
Unlike South Korea, which quickly started testing for COVID-19 using the World Health Organization (WHO) test, the United States refused the WHO test, opting to develop its own through the Centers for Disease Control and Prevention (CDC). But the CDC test was ultimately found to be flawed and represents one of many government stumbles. Without an adequate test, there were nearly 50 days from the first patients in both countries before the United States started to ramp up testing. Why was this so critically important?
During this extended phase in the United States, there were countless numbers of patients presenting with pneumonia and respiratory tract symptoms to emergency rooms, urgent care centers, and doctors' offices. Without the ability to make the diagnosis of COVID-19 or even suspect it, these patients unwittingly spread their infections to healthcare workers. Also, during this first phase of spread, there was likely — albeit still not yet validated — a high rate (approximately 30%) of asymptomatic carriers for COVID-19, which further amplified the chances for doctors and health professionals to be infected.
For the sake of comparison, during the month of February, South Korea performed more than 75,000 tests (versus just 352 in the United States) and adopted all of the WHO best practices, which includes massive testing, tracing every contact of a person infected and testing that person, quarantine of all known cases, and social distancing.
The United States did none of these. Instead, officials repeatedly made bad choices that put public health in jeopardy, along with the healthcare workers charged with caring for the public.
South Korea, meanwhile, got ahead of its outbreak and became a model in the world for how that was achieved. But it wasn't just South Korea that reacted well. As Atul Gawande summarized, Singapore and Hong Kong also adopted all of the WHO practices, including providing protection for their healthcare workers. In both places, healthcare professionals were expected to wear surgical masks for all patient interactions. That practice turns out to foreshadow the second phase of failure in the United States.
The Second Phase: The War Without Ammo
Although Seattle is where the first cluster of cases occurred, it was the unchecked number of patients diagnosed in New York City in early March that led to the full realization of how ill-equipped the country is in terms of personal protective equipment (PPE), intensive care unit beds, and mechanical ventilators.
The dire, inexplicable lack of masks is well recapitulated by Farhad Manjoo in "How the World's Richest Country Ran Out of a 75-Cent Face Mask", and Megan Ranney, MD, MPH, and colleagues similarly describe the profound deficits in PPE and ventilators in a perspective published in the New England Journal of Medicine.
Together, a situation was set up for healthcare workers to not have masks — or to reuse them for days on end — and lack other protective gear. And this is about plain 75 cent masks, not the N95s that are better for blocking aerosol droplets.
But the required sharing of equipment is not just among doctors and nurses; it even extends to patients sharing a ventilator in some intensive care units. To put some numbers on ventilators, we will need several hundred thousand to a million but have fewer than 160,000 throughout the country.
It's bad enough that the United States was totally unprepared for a pandemic and has such an unimaginable shortage of requisite resources. But the situation still gets worse. On a widespread basis, doctors and nurses are being gagged and muzzled by administrators for expressing their concerns, and penalized or even fired when they do speak out.
Meanwhile, the unconscionable lack of COVID-19 testing has continued in this second phase. And with that, systematic testing of the workforce has yet to start, despite being desperately needed.
The Third Phase: Healthcare Professionals Broadly Infected and Dying
Back in Wuhan, Li Wenliang, a 33-year-old ophthalmologist, was one, if not the first, doctor to alert people in China of the outbreak. He died on February 7, 2020. But he certainly wasn't the youngest doctor to die in China. Xia Sisi, a 29-year-old gastroenterologist, also died after a 35-day hospitalization.
Yet on March 11, from the Oval Office, President Trump stated, "Young and healthy people can expect to recover fully and quickly."
By late March more than 54 doctors in Italy had already died, and in the Lombardy region of northern Italy, one of the worst hit regions in the world, 20% of the healthcare workforce have become confirmed cases. Now, in the United States, as large numbers of healthcare professionals are getting diagnosed with COVID-19 in Boston, New York, and other hotspot cities, young doctors are writing their wills and making provisional funeral plans.
COVID-19 was not supposed to kill young people, but young nurses and doctors are dying in the United States. There are many theories as to why this is happening, perhaps the best one is the viral load — the mass of COVID-19 inoculum.
Because healthcare workers are exposed to the sickest patients — often without access to the proper protective equipment — the heavy viral load may be overwhelming even young clinicians' ability to mount a sufficient immune response to counter the infection.
That doctors and clinicians are succumbing to the virus is beyond a tragedy, as many of these dedicated individuals are dying unnecessarily, as a result of the no-testing and no-PPE fiascos.
Yet a far greater toll in numbers is the temporary loss of clinicians to infections and sickness. This is the other poorly recognized exponential growth curve: As each doctor, nurse, respiratory therapist, paramedic, and patient-care person takes care of tens to hundreds of patients at any given time, the loss of even one of these individuals has a dramatic ripple effect on the shortage of professionals trained to care for affected patients, no less the non-COVID-19 usual patient mix. No number of accelerated medical school graduations (which are being announced) can compensate for these losses, not just by numbers but also by experience.
The handling of the COVID-19 pandemic in the United States will go down as the worst public health disaster in the history of the country. The loss of lives will make 9/11 and so many other catastrophes appear much smaller in their scale of devastation. Perhaps what we in the medical community will remember most is how our country betrayed us at the moment when our efforts were needed most.
Eric J. Topol, MD, the editor-in-chief of Medscape, is one of the top 10 most cited researchers in medicine and frequently writes about technology in healthcare, including in his latest book, Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again.
Follow Medscape on Facebook, Twitter, Instagram, and YouTube
Medscape © 2020 WebMD, LLC
Any views expressed above are the author's own and do not necessarily reflect the views of WebMD or Medscape.
Cite this: Eric J. Topol. Topol: US Betrays Healthcare Workers in Coronavirus Disaster - Medscape - Mar 30, 2020.












Comments